

Mpox and the monologics of public health
Mpox and the monologics of public health
Or, why we need a star chart.

Hello all,
This post briefly reflects on the recent Morbidity and Mortality Weekly Report (MMWR) on mpox deaths and infections in the US in the past year. It thinks through what I’m calling public health monologics: a form of thinking that infuses our attachments to a singular disease or infectious agent.
A quick housekeeping thing: As the social media ecology for writing shifts, I’ll be spending more time on Substack Notes. Two ways to join me there: If you’re new to my newsletter, you can subscribe. Also, you can share this post via other channels.
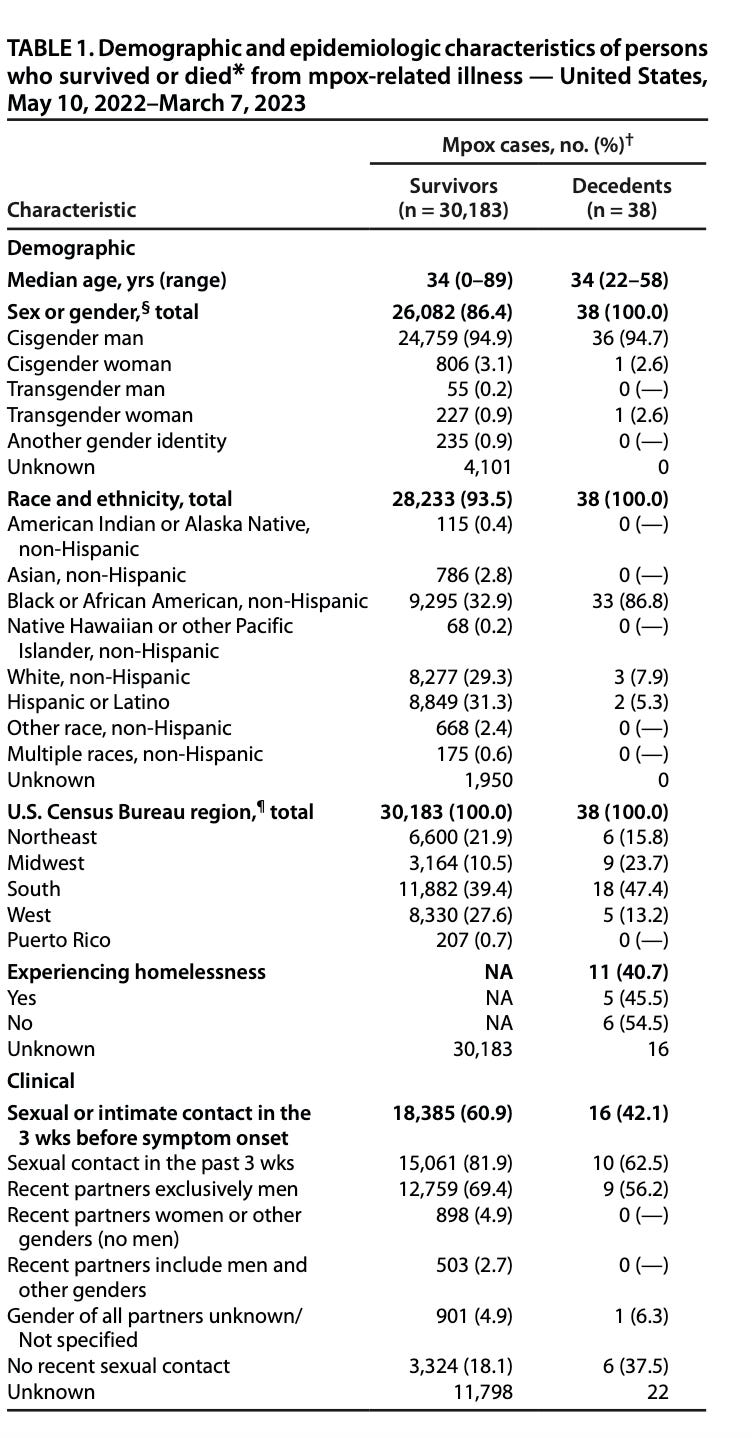
The CDC’s recent Morbidity and Mortality Weekly Report details figures on mpox morbidity and deaths between May 10, 2022 and March 7, 2023.
It denotes that in this time period (and in the context of available data), there were 30,183 people known to have survived infection, and 38 known to have died. Of the 38 who died, 33 were Black — almost 87% of deaths.
Meanwhile, the New York Times ran an opinion piece co-authored by Dan Savage, praising gay men for ending the summer 2022 mpox outbreak. Sorry, correction: Saving us from mpox.
There is no mention of race in the US in the piece.
Let’s look at the CDC MMWR data.
For those for whom this material is new-ish, take a close look at the racial disparities in survival and death in the first table.
Now, look at HIV-related characteristics of those who died from mpox-related illness in the study interval:

Looking at this table, we can see that of the 38 people who died from complications associated with mpox infection, 33 were HIV-positive.
There’s a lesson here, the report states:
The gender and racial disparities in mpox-associated deaths align with previous reports, in which most patients hospitalized for severe manifestations of mpox were Black men with uncontrolled HIV (4) and parallel racial and ethnic disparities in HIV infection and mortality. In 2020, 75% of all-cause deaths among adults with HIV occurred in males, 39% of whom were Black males.**** Disparities and barriers are apparent at all levels of HIV care including recognition of HIV risk, access to testing, and access to and receipt of preexposure prophylaxis and ART (7).
As Joe Osmundson put it, “If you think MPOX is over, ask yourself FOR WHOM?”
Yet HIV remained muted in much of the reflections on mpox in public media. What’s going on with this attachment to one disease?

The challenge here is that addressing one viral outbreak (here, mpox) does not necessarily address the connected issue of un- or under-treated HIV.
This has several implications.
One has to do with the relationship between our social order and our notions of pathology. I dedicated an earlier piece on this newsletter to thinking about this.
Another has to do with the relationship between pathology and care. Consider someone who is HIV-positive, needs antiretroviral treatment for HIV but struggles to access it, and then tests positive for mpox after developing symptoms. Their mpox healthcare encounter could theoretically also route them towards HIV support and care. This is, in fact, what public health programs can do and will do if given the resources: work comprehensively. I like to imagine expansively when it comes to public health. But expansive doesn’t mean the erasure of difference, and differences matter.
“Difference” in the mpox context could be the profound differences in mortality between the thirty-three Black individuals between 22 and 58 years old who died from mpox associated illness, in contrast to two Hispanic/Latino people and three White people.
Difference can also mean differences in available resources. This includes the relative unavailability of the antiviral treatment Tpoxx (Tecovirimat) outside of well-resourced urban centers and/or clinical trial sites. Or the resources to manage the sequelae of untreated mpox illness, including pain and the consequences of pain.
This past year, I was invited to a workshop at Georgetown Law on mpox and health policy. To me, the most interesting and compelling talks came from people representing Pride organizations and nonprofit HIV care centers in the South. They explained how Covid stretched their labor paper-thin. Sure, we could have conversations about what they might be doing to incorporate mpox awareness and vaccination into Pride parades, HIV support groups, or social media. But what they emphasized was clear: already facing the racialized disparities in HIV/AIDS infection among their client communities, they were now being tasked by local public health officials to add mpox vaccination and care to their responsibilities.
The difference at stake was actually a difference in care’s visibility. They warned about the enduring indifference to Black illness and death in the American public imagination, and the public’s indifference to the labor of nonprofit workers and volunteers, to mitigate risks of that illness and death. Both matters, they said, were being made invisible now that the summer’s initial waves of cases were on the decline.
After all, they explained, payroll doesn’t magically expand to accommodate more trained counselors, or vaccinators, or hotline staffers. The thing about a public health emergency is that things can’t just be straightforwardly outsourced to community-based organizations...but it often is. That’s the structure of American public health emergencies, far too often.
The challenges stemming from the CDC report, then, are manifold. The sources of support to implement its lessons are at risk of disappearing. Judicial rulings that may limit access to preventative health services (especially for PrEP), and the recently-announced end to the federal Public Health Emergency (PHE) for Covid-19, slated for May 11, present as-yet untold ripple effects. The moral imagination of health in the US is still tied to emergency in a monologic mode, too often focused on one problem at a time.
We have seen this monologic in many public health contexts. It’s an attachment to the idea that bodies can be reducible to one infectious agent’s presence or absence. Covid certainly did not cause this mode of thought, but “magic bullet” thinking intensified during the pandemic and still shades popular understandings of illness, health, and risk. This is especially true when it comes to sexually-transmitted diseases, something that would be fraught with mpox because of the tussle between naming it as an STD versus a disease of “contact.”
The one-disease-one-body thinking endures as a public health logic. Covid is still with us on this front. From headlines such as “Mpox has faded in the U.S. Who deserves the credit?” to framings declining mpox case counts as “a mystery” to be answered by a singular solution, there’s a bad attachment here to the fading of an outbreak and the search for a singularities. Out of sight, out of mind, enter the heroes, now we see (one thing, not others).
What are the consequences of this overfocused visibility? Some experts suggest zooming out via re-doubled efforts at mpox vaccination. The idea here is broadened protections against a potential wave of infections this summer. This could occur in a moment when, as of April 26, 2023, the 7-day average number of cases is zero. (The number of new cases of HIV in the US is most certainly not zero.)

I certainly support this effort.
At the same time, we also know that the gendered and racial disparities in deaths from mpox are not isolated from, but continuous with HIV infection risks. Mpox and HIV could never be considered apart. Bodies register this enduring tie, and the mortality story of mpox is one not of generic bodies. It is a one of bodies unequally exposed to the racist and classist forces that exacerbate viral exposures. Vaccination’s possibilities and pitfalls must to be understood in the same way. The CDC gets this, when it comes to thinking about multiple disease risks and their attendant prevention strategies. The lesson here is the need to shift towards the plural, generating possibilities for more — rather than less — visibility and care for those whose lives are most on the line.
Monologics risk the overproduction of singularities, too-simple stories about bodies and threats. We’re seeing the proliferation of reductive social disease models that cannot and will not address our pathological social order.
The whitewashing of mpox into a story of being over and done by heroic gay men exemplifies one such singularity. The lure of a solo hero narrative (even when tendered as a group effort) is that it might carry us from the dread of chaotic emergency to the comfort of ordered success. Lines are tempting because they promise transition, and plot a way through the constellation of difference. The line promises deliverance to the story’s end.
But the constellation is the story of mpox. It’s a constellation that includes HIV’s racialized transmission dynamics on one hand, the increasing restrictions on HIV prevention and treatment access on the other, and the enduring forms of desire and aversion that underpin both.
We need a star chart, not a pinhole telescope, as we look towards the summer skies.